
Let me paint a picture: You’re in the Emergency Department at 2 a.m., flipping through troponins and chasing ECGs like a caffeine-fueled cardiophile… and then, there it is — ST elevation, apical ballooning on echo, coronaries clean as a whistle. Your inner Sherlock mutters: “It’s not a heart attack… it’s heartbreak.” 💔
Welcome to the emotionally dramatic world of Takotsubo Cardiomyopathy — a condition that looks exactly like an MI, behaves like an MI, but isn’t an MI. Also known as Stress-Induced Cardiomyopathy, it’s what I call the real-life plot twist of the CCU.
But before we dive into this mnemonic, let’s first understand what it really is:
💡 What Is Takotsubo Cardiomyopathy?
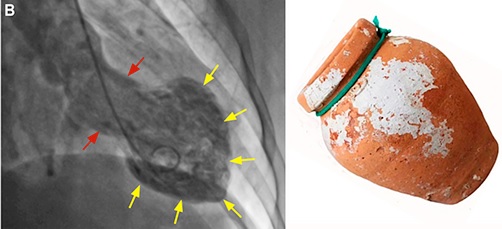
A transient, reversible LV dysfunction usually triggered by severe emotional or physical stress — hence the nickname “Broken Heart Syndrome.”
Named after a Japanese octopus trap (:D yes, really), due to the ballooned-out shape of the LV on echo.
Takotsubo Cardiomyopathy Mnemonic – “BROKEN”
| Letter | Represents | Explanation |
|---|---|---|
| B | Ballooning (Apical) | Classic echo finding – apical ballooning, mimicking anterior MI. |
| R | Reversible | LV dysfunction typically recovers in days to weeks. |
| O | Often Post-Stress | Emotional trauma, surgery, illness — the trigger is usually dramatic. 😩 |
| K | Klean Coronaries | Angiography shows no obstructive coronary artery disease. |
| E | ECG Mimics STEMI | ST elevation, T wave inversion, QT prolongation — but no infarct. |
| N | Non-Ischemic Pattern on MRI | Cardiac MRI: no late gadolinium enhancement (helps differentiate from MI). |
🩺 Clinical Pearls from the CCU (Quetta Chronicles)
I still remember a middle-aged lady we admitted during Eid, classic story — sudden chest pain after hearing her son was in an accident (he turned out fine). Troponins were mildly up, ECG screamed STEMI, echo looked like the heart was auditioning for a balloon animal contest. But angio? Clean.
Takotsubo. We treated supportively and watched her LV recover like a champ within 2 weeks.
Moral of the story: Always suspect Takotsubo when ECG is loud but angio is innocent.
🔍 Key Points for Exams & Wards
- Common in postmenopausal women.
- Troponins may be mildly elevated.
- Manage like ACS initially (you won’t know it’s Takotsubo right away).
- Beta-blockers + supportive care; avoid inotropes if LVOT obstruction present.
- Watch for complications: heart failure, arrhythmias, LV thrombus.
I hope that you find this medical useful in your studies/clinical practice. Happy learning! 🙂
Authored by:
Dr. Aurangzaib Qambrani
MBBS | PLAB | MRCP-UK
General Medicine, Gastroenterology & CCU
Sheikh Khalifa Bin Zayed Hospital, Quetta 🏥




 Management Mnemonic")


")
")


















")
")

{kind=link}